
Airway Management: Options for Airway Management
There are four primary options:
- Face mask
- Supraglottic airway
- Endotracheal tube
- Surgical airway
Before attempting any airway intervention, a thorough check for necessary equipment is necessary. A mnemonic that can be used to check your equipment is SLOPESSS:
- Suction
- Laryngoscope
- O2 source
- Positive pressure (ventilator or Laerdal bag)
- Endotracheal tube
- Stylet
- Syringe
- stethoscope/CO2 detector
Before any medications are given, the patient should be pre-oxygenated with 100% oxygen.
Face Mask
Examples include simple face mask with titrated oxygen flow, non-rebreather mask, and Laerdal bag mask. The first two can provide supplemental oxygen but cannot assist with ventilation. Bag mask ventilation can be achieved with a Laerdal bag. An oropharyngeal airway or nasal pharyngeal airway may be used to bypass the soft tissues of the oropharynx when performing bag mask ventilation.
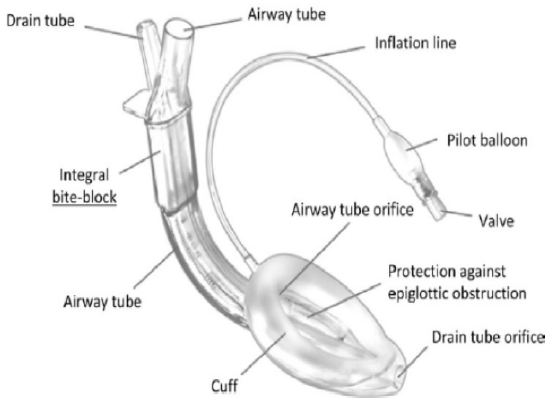
Supraglottic Airway Device
The Laryngeal Mask Airway (LMA) is a commonly used supraglottic airway device. These devices provide a seal over the laryngeal inlet. They can be used in a number of surgical procedures under general anesthesia and can also be used as an advanced airway intervention in the ACLS algorithm. The biggest concern with supraglottic airway devices is its relative inability to protect from aspiration compared to an endotracheal tube, although newer models of LMAs may have a gastric port that provides an outlet for gastric contents.
Some traditional relative contraindications include lack of familiarity with the device, patients at increased risk for aspiration in an elective setting (see chapter on preoperative assessment for risk factors for aspiration), compromised positioning such as prone cases, laparoscopic surgeries, and pregnant patients.
Endotracheal Tube
An endotracheal tube (ETT) can be placed with the use of direct laryngscopy, with video laryngoscopy, or with a bronchoscope. Direct laryngoscopy is most successful with optimal positioning and requires some degree of neck mobility. In patients with restricted neck mobility or neck pathology (ex trauma patients in c-spine collars), intubation with video laryngoscopy or a bronchoscope may help minimize neck movement.
The size of an ETT refers to its internal diameter. As a general rule, adult females are typically a size 7 – 7.5mm tube, while adult males are typically a size 8 – 8.5mm tube. A stylet can be inserted into the ETT to give it more shape during intubation. This style is removed as the tube is advanced through the vocal cords.
The insertion of the ETT should be visualized. Other ways to confirm the placement of the tube into the trachea is to look for bilateral chest rise, lung auscultation, misting of the ETT, and an end tidal CO2 tracing on the monitor of the anesthesia machine.
A cuffed endotracheal tube provides the most protection against aspiration.
In general, there are five indications for endotracheal intubation: inability to maintain airway patency, inability to protect the airway against aspiration, failure to ventilate, failure to oxygenate, and anticipated deterioration in clinical course.
Surgical Airway
A surgical airway may be established in a planned or emergent fashion. If the patient cannot be oxygenated or ventilated with any of the aforementioned methods, and a return to spontaneous ventilation cannot be quickly established, an emergent surgical airway may be necessary. Alternatively, this may be a planned procedure, such as in a patient undergoing complex oral or craniofacial surgery.
The primary site of entry for a surgical airway is the cricothyroid membrane. The cricothyroid membrane is between the thyroid and cricoid cartilages. The thyroid cartilage (the “Adams apple”) is the most prominent aspect of the anterior neck and provides a landmark for a surgical airway. Caudal to the thyroid cartilage the cricothyroid membrane. The “scalpel-bougie-tube” technique is recommended as the preferred method, where an incision is made with a scalpel, a bougie is advanced into the trachea via the incision, and an ETT is advanced over the bougie.
Next page: Difficult Airway Algorithm
Previous page: Anatomy