
Resuscitation: Important considerations
The Key to survival from VF/pulseless VT is good, early CPR and early defibrillation!
The Key to survival from PEA/Asystole is good, early CPR and excluding all reversible causes
Other considerations:
- If you are alone, your priority is to deliver chest compressions.
- Effective CPR provides 25-33% of normal cardiac output.
- The aortic diastolic pressure (AoDP) is critical to coronary artery perfusion and rises in a gradual manner. Therefore, chest compressions should continue uninterrupted.
- Bradyarrhythmias of most concern are Mobitz Type 2 and 3rd degree heart block as both can degenerate to asystole.
- No drug given during ACLS has been shown to increase survival
- May provide epinephrine, atropine, lidocaine and naloxone through ETT if no IV/IO.
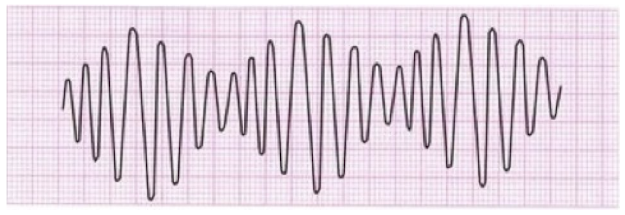
- Magnesium (1-2 g bolus over 10-20 mins) is used as an anti-arrhythmic for torsade de pointes, a form of VT (see Figure 1)
- Head tilt and chin lift should be avoided if cervical spine injury is suspected.
FIGURE 1 - TORSADE DE POINTES VENTRICULAR TACHYCARDIA.
Next page: Special Circumstances